
Anemia and Malaria
In malaria endemic regions, being anemic could be keeping children safe

Over half of children under five in sub-Saharan Africa have anemia, an illness that can cause permanent developmental delays and be fatal if left untreated. Anemia, which is often caused by iron deficiency, is a condition marked by a lack of healthy red blood cells, which carry oxygen throughout the body. The resulting deprivation of oxygen to vital organs can impair cognitive performance, growth and development, cause extreme fatigue, increase the risk of infection, and raise the risk of premature birth. Left untreated, it can be life threatening.
The cure should be simple and relatively cheap: iron supplements. The WHO set a goal of halving the prevalence of anemia in women of reproductive age between 2012 and 2025. There is one unintuitive wrench in these plans: providing iron supplements to anemic populations might actually worsen their overall health and life expectancy.
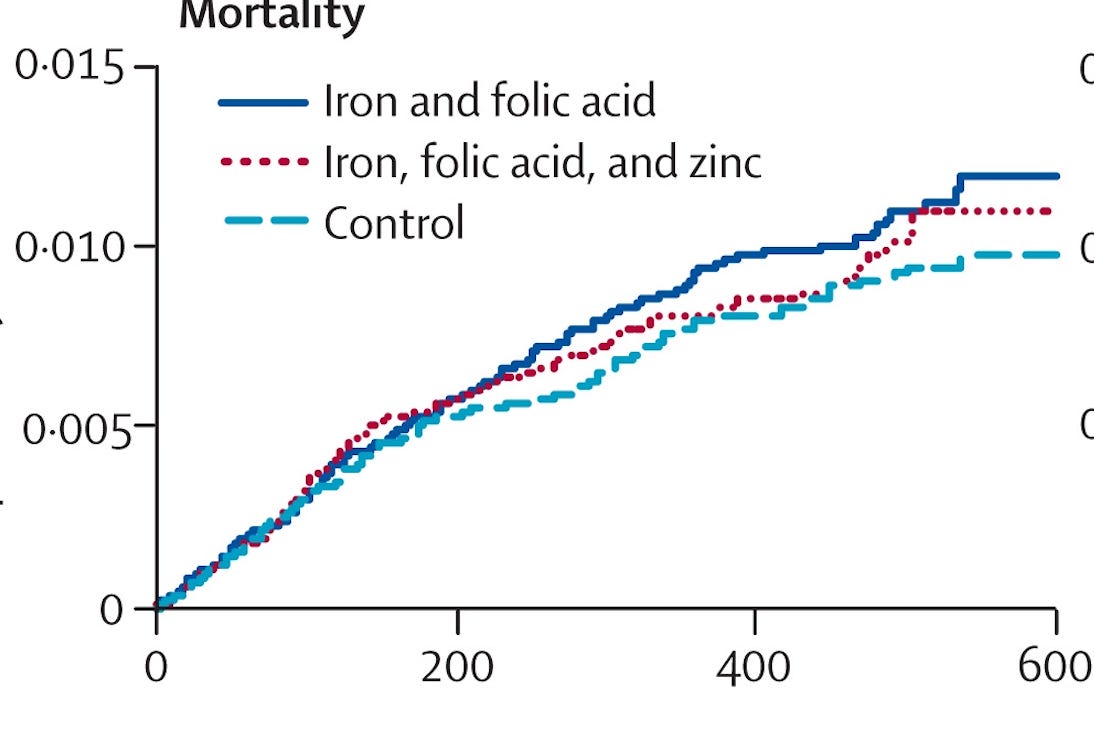
In 2003, researchers launched a randomized control trial to measure the health impact of iron and folic acid supplementation among preschool aged children on Pemba island in Zanzibar. The intervention was set up to measure how much health outcomes among children improved as a result of supplementation. However, the study was abruptly shut down when the intervention group, which received a daily iron dose, were 11 percent more likely to be hospitalized and 12 percent more likely to die from severe illness compared with those who did not receive treatment.
Some researchers suspect that malaria is the reason for the surprising results. Sarah Cusick, an Associate Professor of pediatrics at the University of Minnesota School of Medicine whose research focuses on nutritional deficiencies points out that ‘Pemba island is in an intense area of malaria transmission and, at the time, the government was doing very little for malaria control – no spraying, no nets – so it was intense year-round malaria transmission. What really implicated malaria is that the same researchers did a parallel study in Nepal and there was no harmful effect of iron.’ Cusick conducted her doctoral research on a sub-study of the Pemba RCT.
So far, there is not much evidence, but some later studies have supported the finding that, in areas where malaria is prevalent and without robust prevention and control systems, iron supplementation can increase malaria risk, which is worse for outcomes than iron deficiency anemia. ‘This came as a surprise to almost everyone’, says Chandy John, a Professor of Medicine at Indiana University whose research focuses on malaria.
The group of parasites that cause malaria are dependent on iron to proliferate. As a result, some evidence suggests that being iron deficient or anemic offers protection against malaria infection. In a 2012 study, researchers followed a cohort of 785 Tanzanian children over three years and found that those who became naturally iron deficient were 60 percent less likely to die than those who did not.
This relationship is especially problematic because, if it is true, it might work both ways: just as iron deficiency appears in some evidence to protect against malaria, other evidence implies malaria itself increases the risk of iron deficiency. This is part of the reason places with endemic malaria have higher rates of anemia, on average, than those without. A 2015 study of children under 5 years old in Kenya finds that the prevalence of iron deficiency in children decreased significantly after a one-year interruption of malaria transmission.
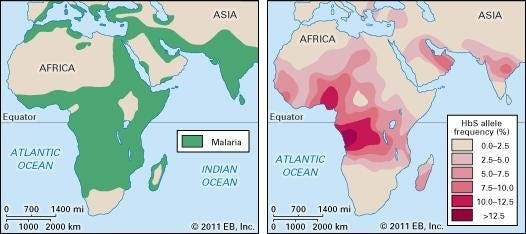
Malaria is so dangerous that it can be evolutionarily ‘worth’ extremely high rates of life-threatening diseases to avoid. This is why sickle-cell anemia and beta thalassemia are more prevalent in malarial areas: having one copy of the recessive gene is protective.
As of 2023, the WHO says ‘progress on reducing anemia has been slow and the world is not on track to reach the global target.’ The problem of iron deficiency is inherently linked to the complex challenge of controlling and eradicating malaria: not only because of the troubling suggestion it may be unsafe to address iron deficiency unless paired with malaria control, but also because ‘kids absorb twice as much iron if you treat their malaria first’, according to Cusick.
Good malaria prevention through bed nets, responsive diagnostics, and good treatment capabilities mitigates any risks potentially associated with iron supplementation. Thankfully, therefore, recent developments bring good news: fifteen African countries are expected to deploy the R21 malaria vaccine – the second ever to be recommended by the WHO –- this year. Compared to the current vaccine, the R21 vaccine is more effective, and is the first to meet the WHO’s goal of 75 percent efficacy.
These findings are an illustration of the unexpected effects of even straightforward health interventions, when applied to new settings where evidence is far from perfect and comprehensive. We need more evidence to resolve this question, make global health efforts more effective and reduce the tragedy of child mortality.
 | A guest post by
|